

Credits
Host: Sara Dong
Guest: Justin Penner
Producing/Editing/Cover Art: Sara Dong
Our Guest
Justin Penner, MD, FRCPC, MSc, DTMH, MRCPCH

Justin completed his medical school and paediatric residency at the University of Manitoba in Winnipeg, Canada. Always having an interest in infectious disease, he subsequently completed an MSc in tropical medicine and international health at the London School of Hygiene and Tropical medicine followed by a fellowship in paediatric infectious diseases at St Mary’s Hospital in London, UK and a fellowship in paediatric immunocompromised ID at Great Ormond Street Hospital. Justin is a member of the PENTA network educational group on congenital infections and has a particular interest in indigenous health in the Canadian North. He currently works as a paediatric infectious diseases consultant at the Children’s Hospital of Eastern Ontario in Ottawa, Canada and at the Qikiqtani General Hospital in Iqaluit, Nunavut and as an honourary academic fellow at Great Ormond Street Hospital.
Consult Notes
This episode kicks off our Curious Congenital Conundrums series that will run in April and May 2022! Please check out these upcoming episodes below!
| Release Date | Title | Host | Discussant(s) |
| April 4 | Febrile Digest – Think SCORTCH + Curious Congenital Conundrums Introduction | Dr Sara Dong | Dr Justin Penner (Children’s Hospital of Eastern Ontario & Great Ormond Street Hospital) |
| April 11 | Curious Congenital Conundrums – Stop, Look, and Listen | Dr Nuria Sanchez-Clemente (London School of Hygiene & Tropical Medicine, London, UK) | Dr Hemione Lyall (St Mary’s Hospital, Imperial College London Healthcare Trust, London, UK) |
| April 25 | Curious Congenital Conundrums – Seal of Approval | Dr Ella Dzora (Sheffield Children’s Hospital, Sheffield UK) | Dr Jason Brophy (Children’s Hospital Of Eastern Ontario, Ottawa, Canada) |
| May 9 | Curious Congenital Conundrums – In the Eye of the Beholder | Dr Carsten Krueger (Children’s Hospital of Eastern Ontario, Ottawa, Canada) | Dr Clare Nourse (Queensland Children’s Hospital, Brisbane, Australia) Dr Justin Penner (Children’s Hospital of Eastern Ontario & Great Ormond Street Hospital) |
| May 23 | Curious Congenital Conundrums – A Cold Sore Crisis | Dr Sarah-May Johnson (Great Ormond St Hospital, London, UK) | Dr Fani Ladomenou (Venizeleion General Hospital of Heraklion, Crete, Greece) |
We spent the rest of the episode discussing the SCORTCH framework!
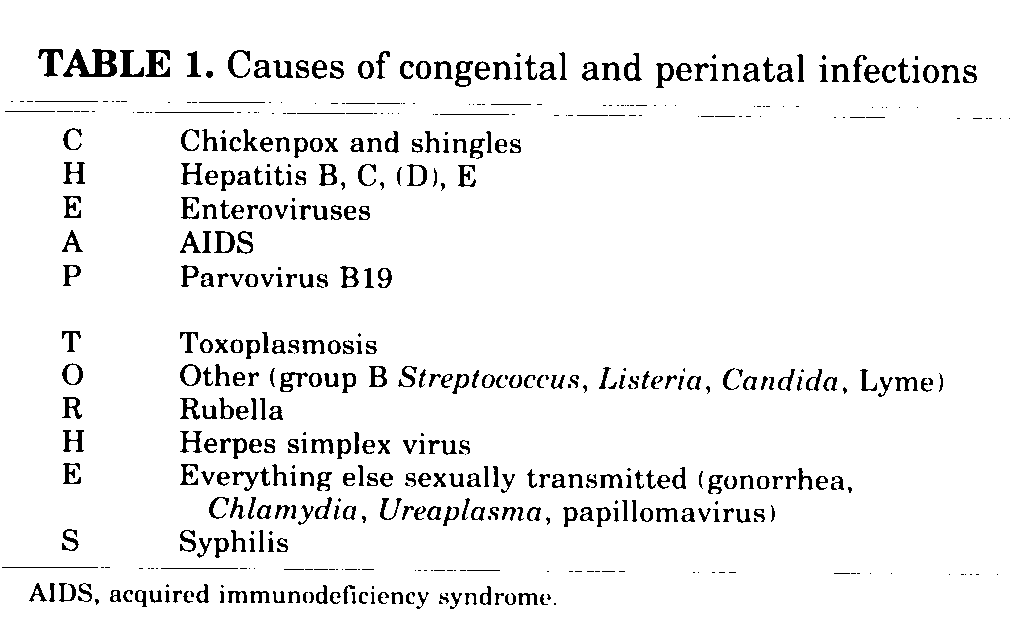
Many of us have been taught or learned the classic “TORCH” mnemonic for congenital infections:
- T = toxoplasmosis
- O = other
- R = rubella
- C = CMV
- H = HSV
From the best I could tell, the TORCH/TORCHeS acronym originated in the 1970s and has been attributed to Dr. Nahmias from this article: Nahmias, A., Walls, K., Stewart,, J. et al. The ToRCH complex-perinatal infections associated with toxoplasma and rubella, cytomegol- and herpes simplex viruses. Pediatr Res 5, 405–406 (1971). https://doi.org/10.1203/00006450-197108000-00144
Over time, this acronym became more outdated and “SCORTCH” isn’t the first push to consider variations to this approach. There have been some papers that demonstrate that relying on just “routine TORCH serologies” for diagnosis has poor diagnostic return, and Justin emphasized this by pointing out how we have multiple modalities for diagnosis to consider now and changing epidemiology.
- Leland D, French ML, Kleiman MB, Schreiner RL. The use of TORCH titers. Pediatrics. 1983;72(1):41-43.
- de Jong EP, Vossen AC, Walther FJ, Lopriore E. How to use… neonatal TORCH testing. Arch Dis Child Educ Pract Ed. 2013;98(3):93-98. doi:10.1136/archdischild-2012-303327
But it’s hard to get rid of acronyms altogether. Here is one that tried to suggest “cheap torches”: Ford-Jones EL, Kellner JD. “Cheap torches”: an acronym for congenital and perinatal infections. Pediatr Infect Dis J. 1995;14(7):638-640.
Which then bring us to SCORTCH. Check out this overview and the associated graphics in this article: Penner J, Hernstadt H, Burns JE, Randell P, Lyall H. Stop, think SCORTCH: rethinking the traditional ‘TORCH’ screen in an era of re-emerging syphilis. Arch Dis Child. 2021;106(2):117-124. doi:10.1136/archdischild-2020-318841
Here is an additional Viewpoint as well: Fifer H, Hughes G, Ladhani S. Shining the light on congenital syphilis: from TORCH to SCORTCH. Arch Dis Child. 2021;106(10):937-938. doi:10.1136/archdischild-2019-318503
In the paper above and on the episode, Justin talked a bit about “SCORTCH”:
- S = syphilis
- C = CMV
- O = other
- R = rubella
- T = toxoplasmosis
- C = chickenpox (varicella zoster virus)
- H = HSV and others
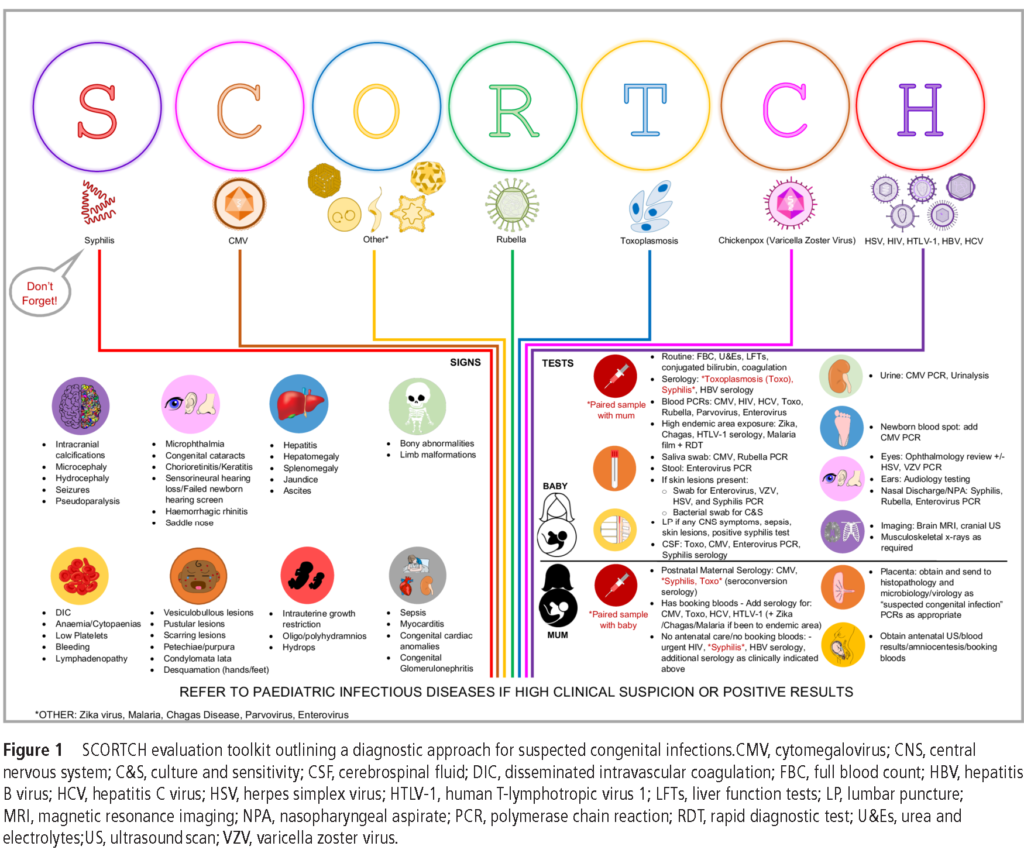
I had Justin talk through the O and H buckets, since these encompass multiple pathogens.
- O includes Zika, malaria, chagas disease, enterovirus, parvovirus – but also leaves a space to insert new infections as needed in the future
- H includes various blood-borne viruses including HIV, hepatitis B, hepatitis C, HTLV-1
A few points from the episode:
- The classic ‘TORCH” screen often fails to incorporate important diagnostic tests by emphasizing serology specific testing and it has the potential to miss key diagnoses, especially emerging/re-emerging infections
- The absence of S often leads to a lack of consideration for congenital syphilis, and syphilis rates have been rising in many countries, particularly heterosexually acquired infections in women of child bearing age.
- Using SCORTCH provides a way to emphasize syphilis testing, but is also a reminder to help advocate for consideration of other possible antenatal infections
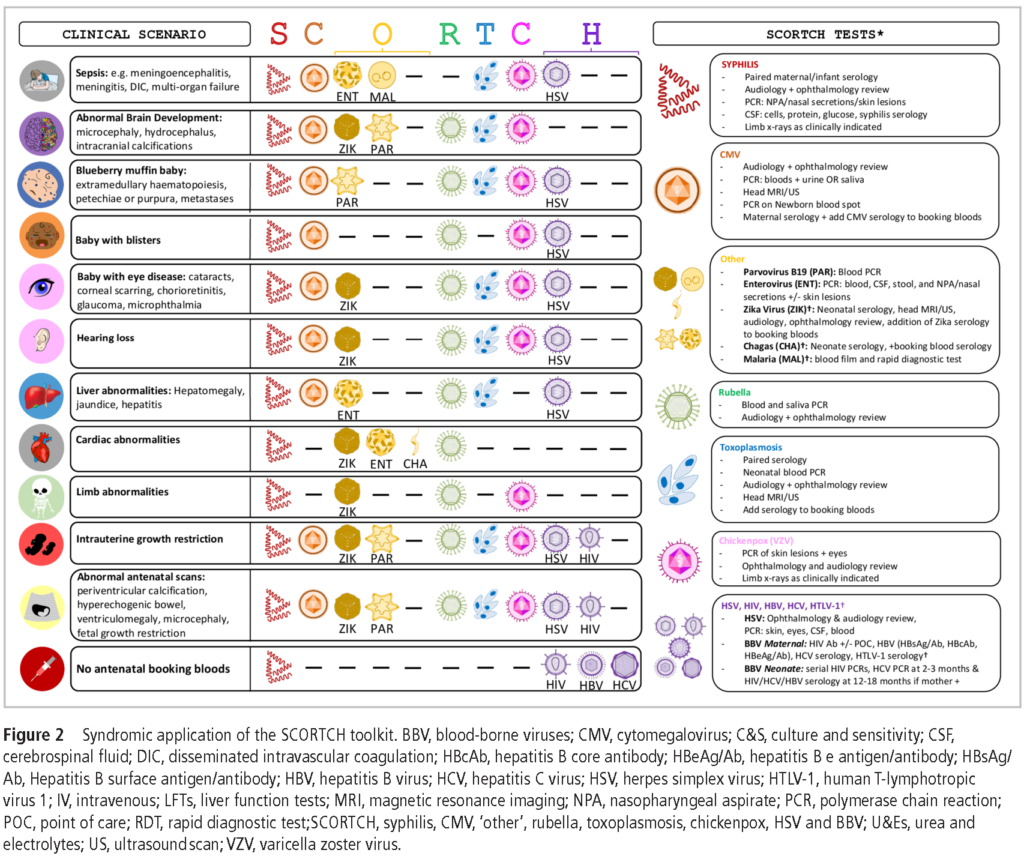
- Congenital infections often have overlapping clinical presentations!
- We need a high index of suspicion
CCC Series Art & Infographics
Disclosures
Our guest (Justin Penner) as well as Febrile podcast and hosts report no relevant financial disclosures
Citation
Penner, J., Dong, S. “#36: Febrile Digest – Think SCORTCH + Curious Congenital Conundrums Introduction”. Febrile: A Cultured Podcast. https://player.captivate.fm/episode/6f5250e0-4fd1-4e00-bb22-e4a919b74291